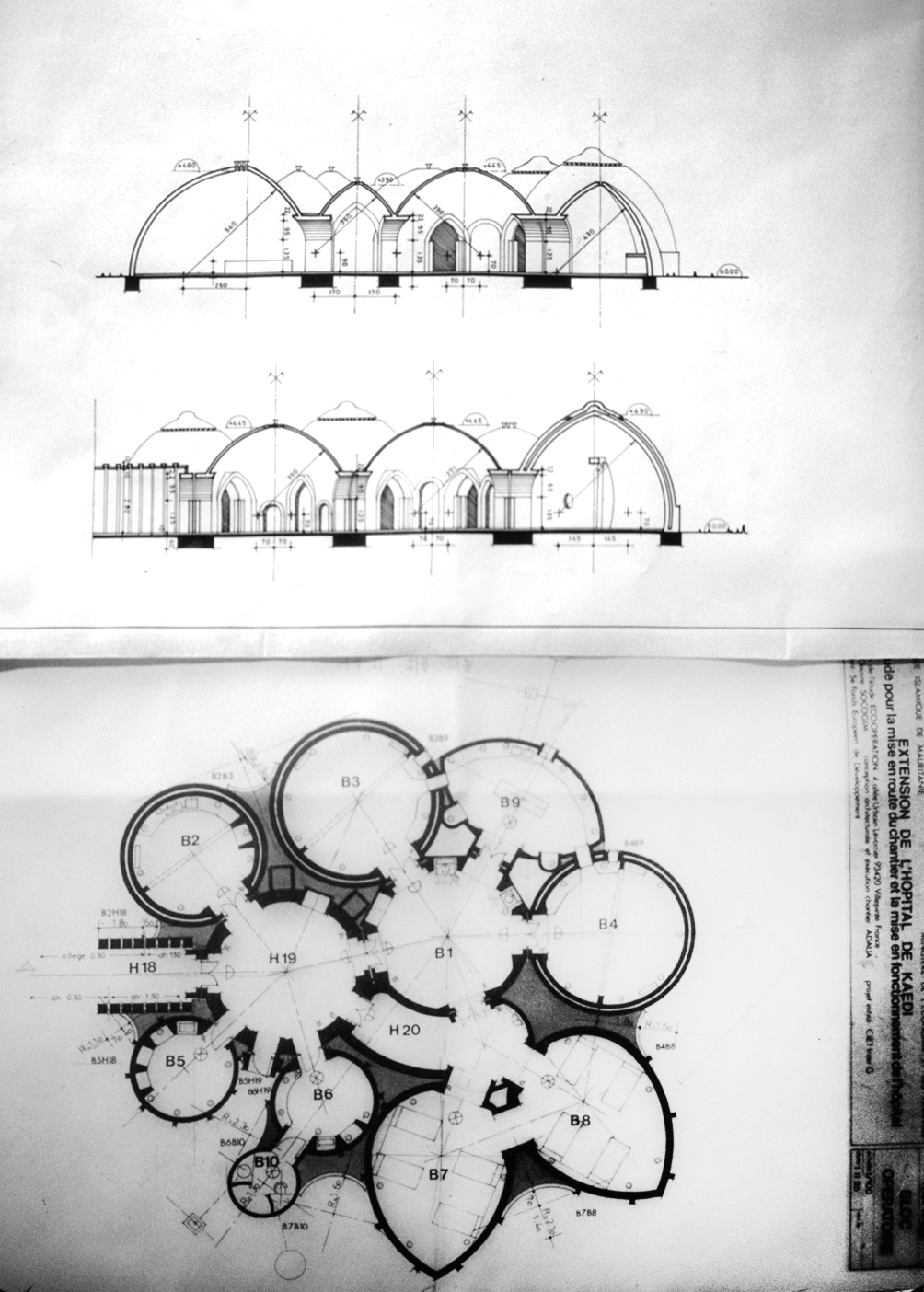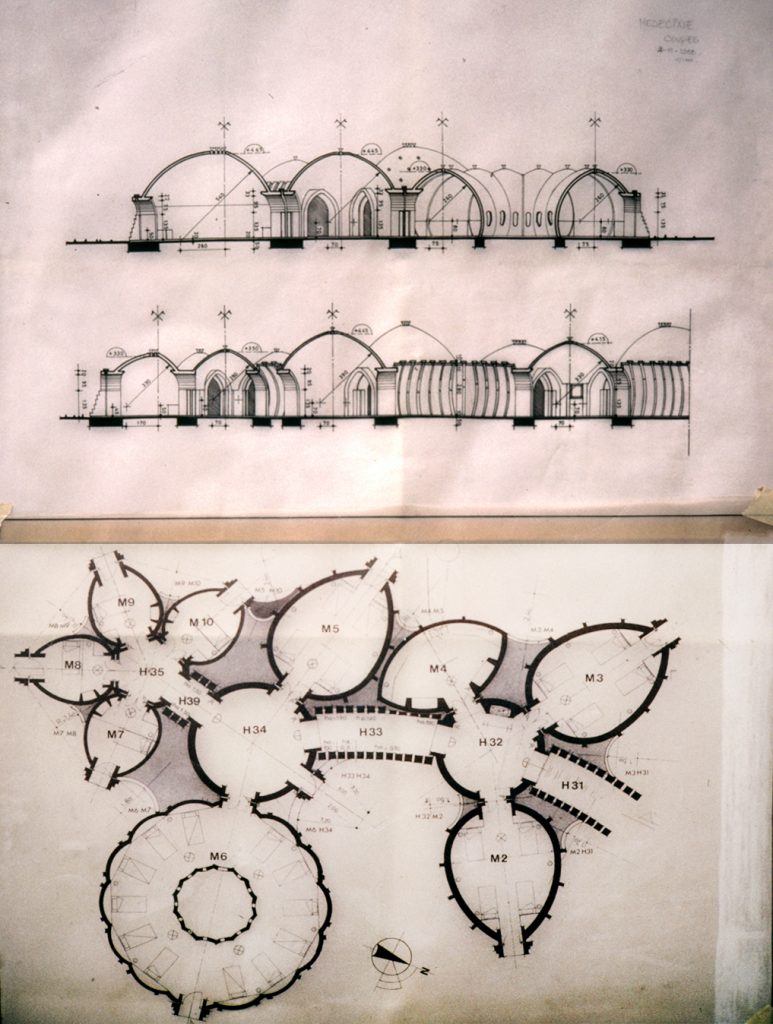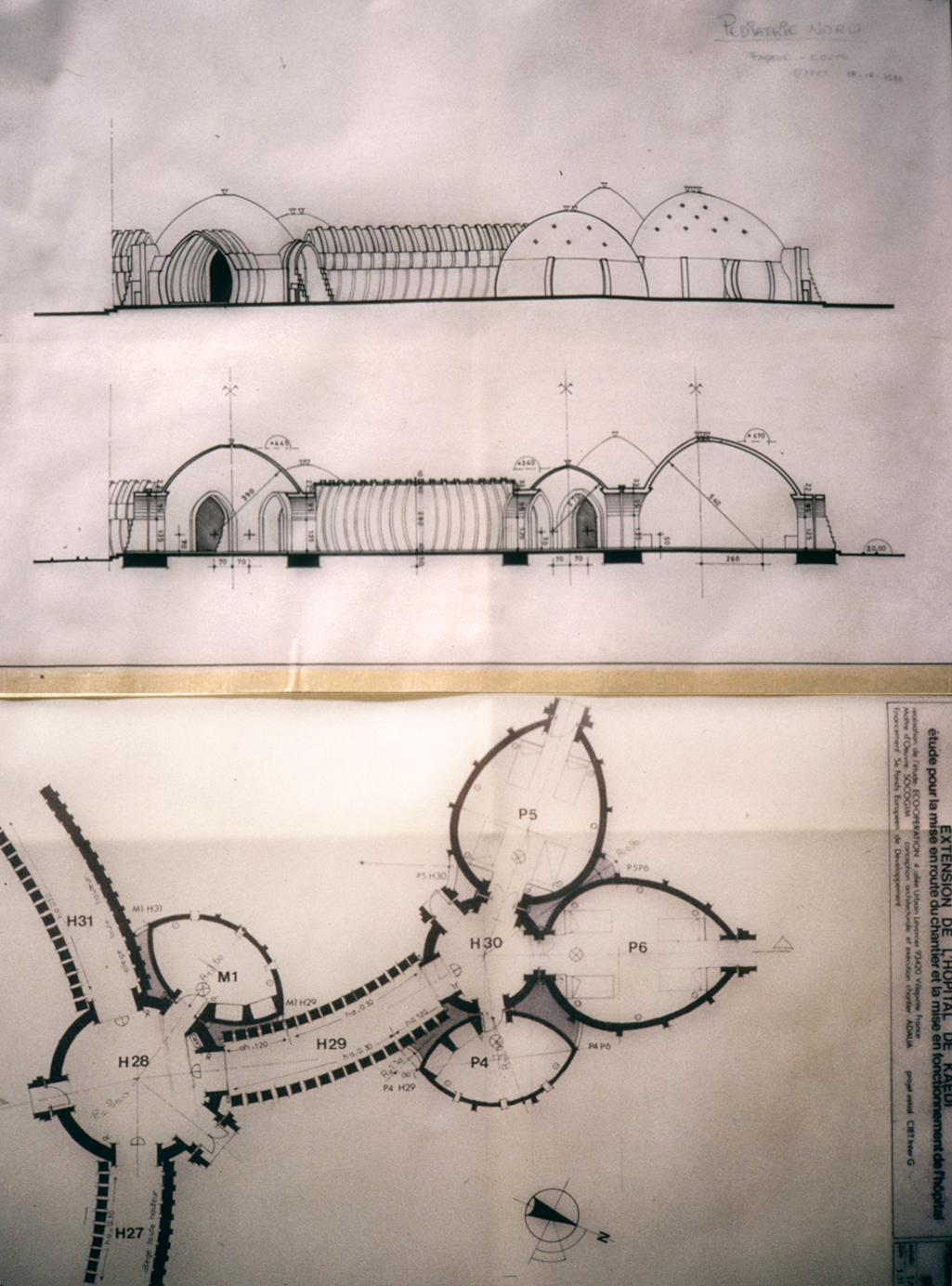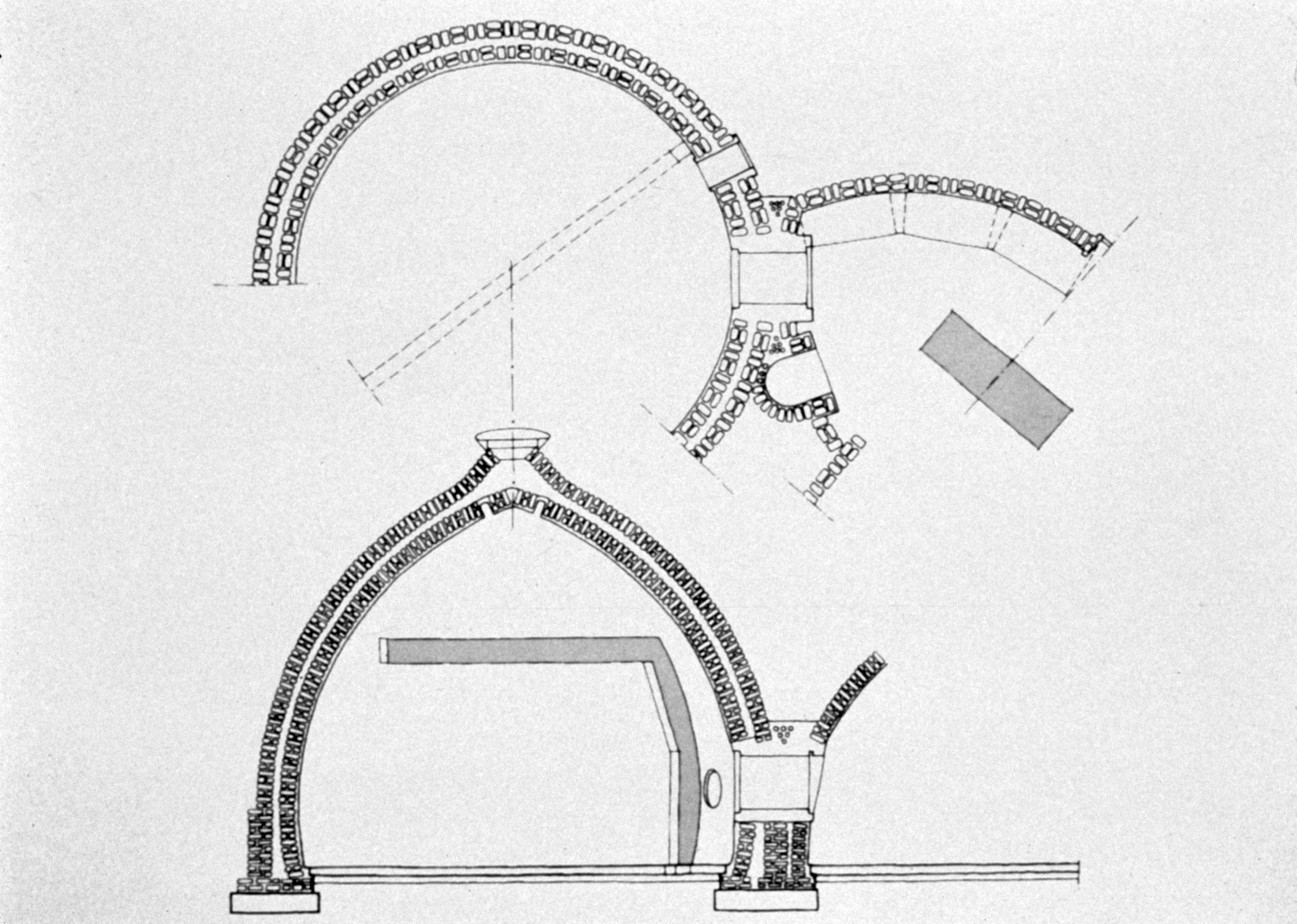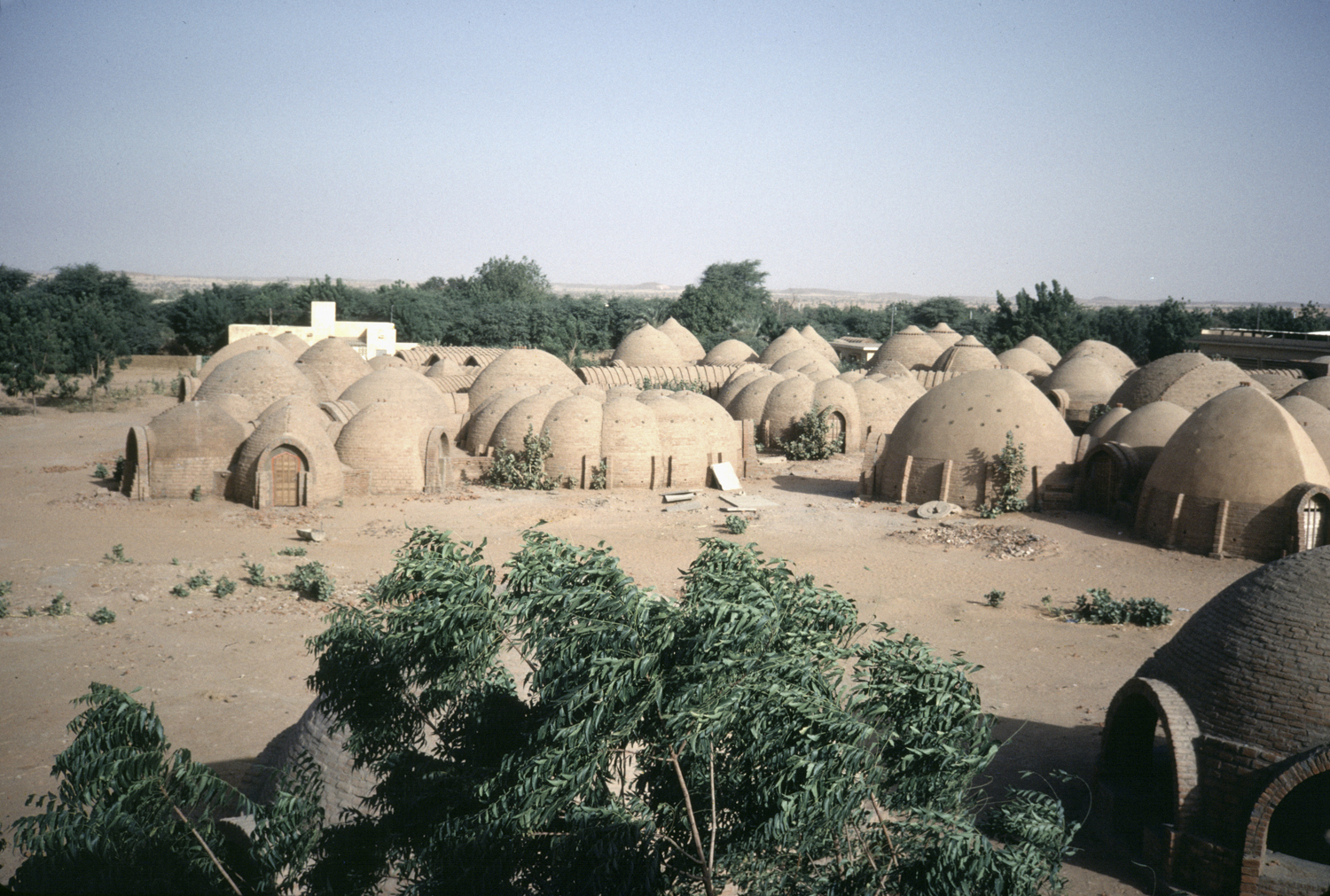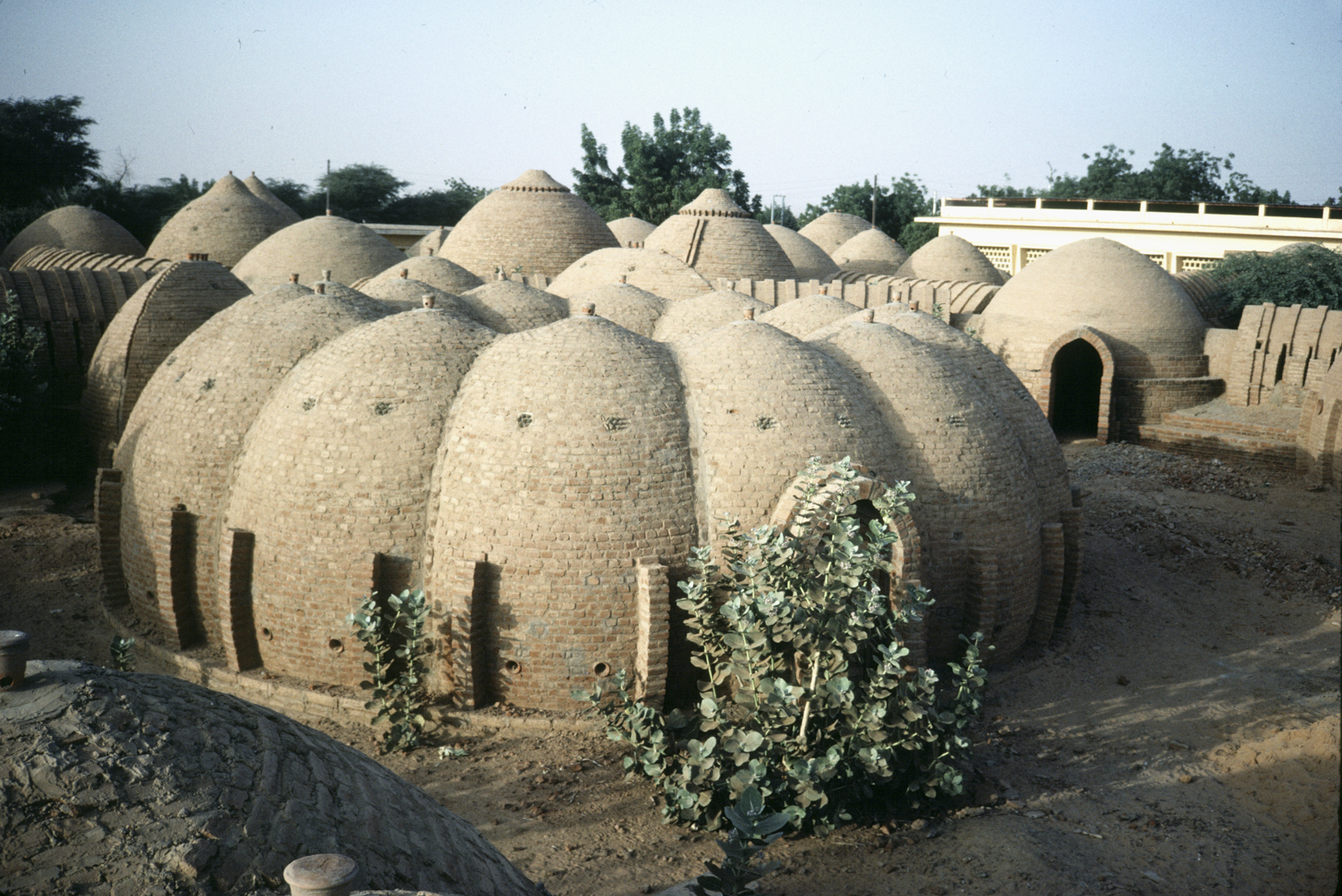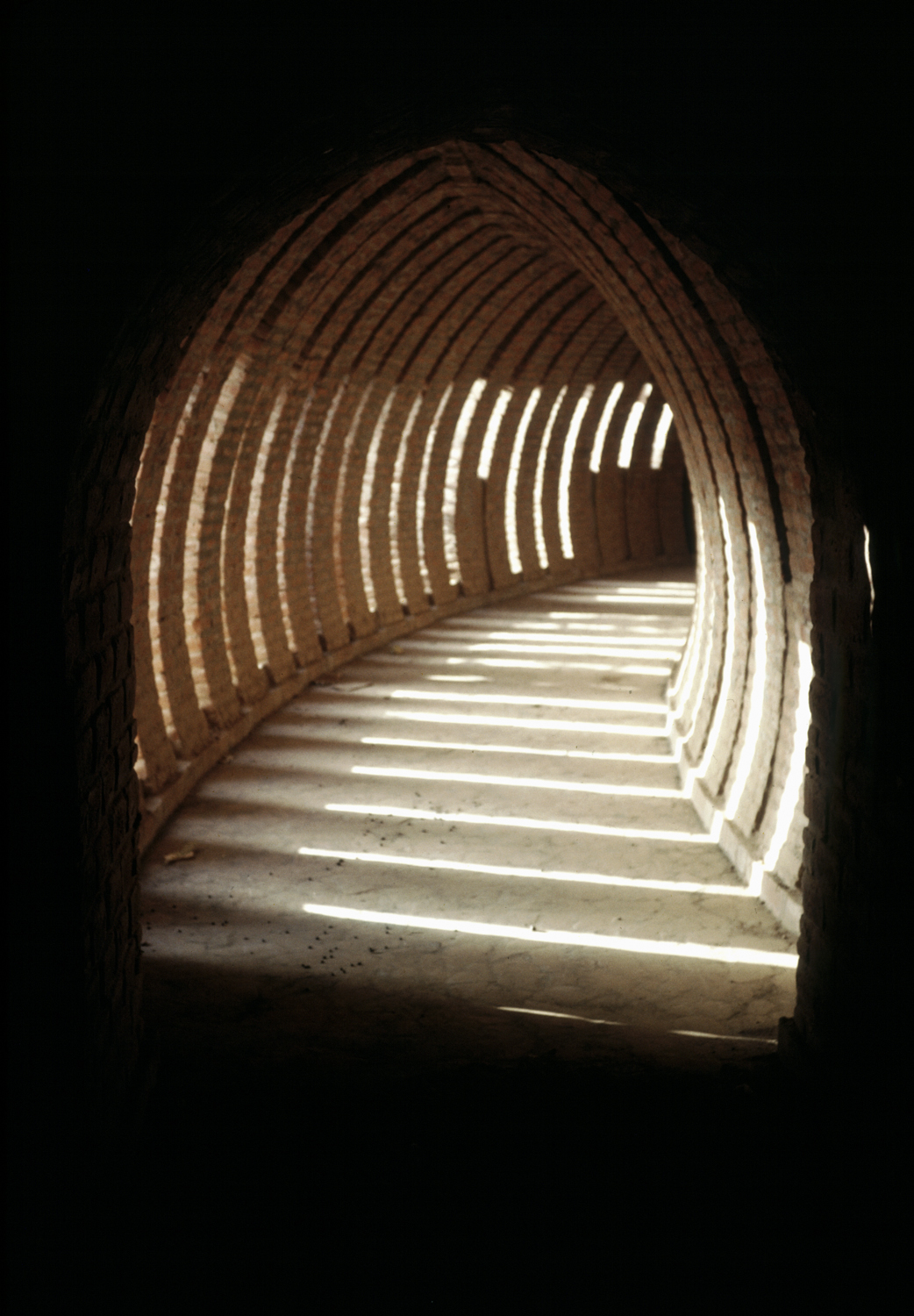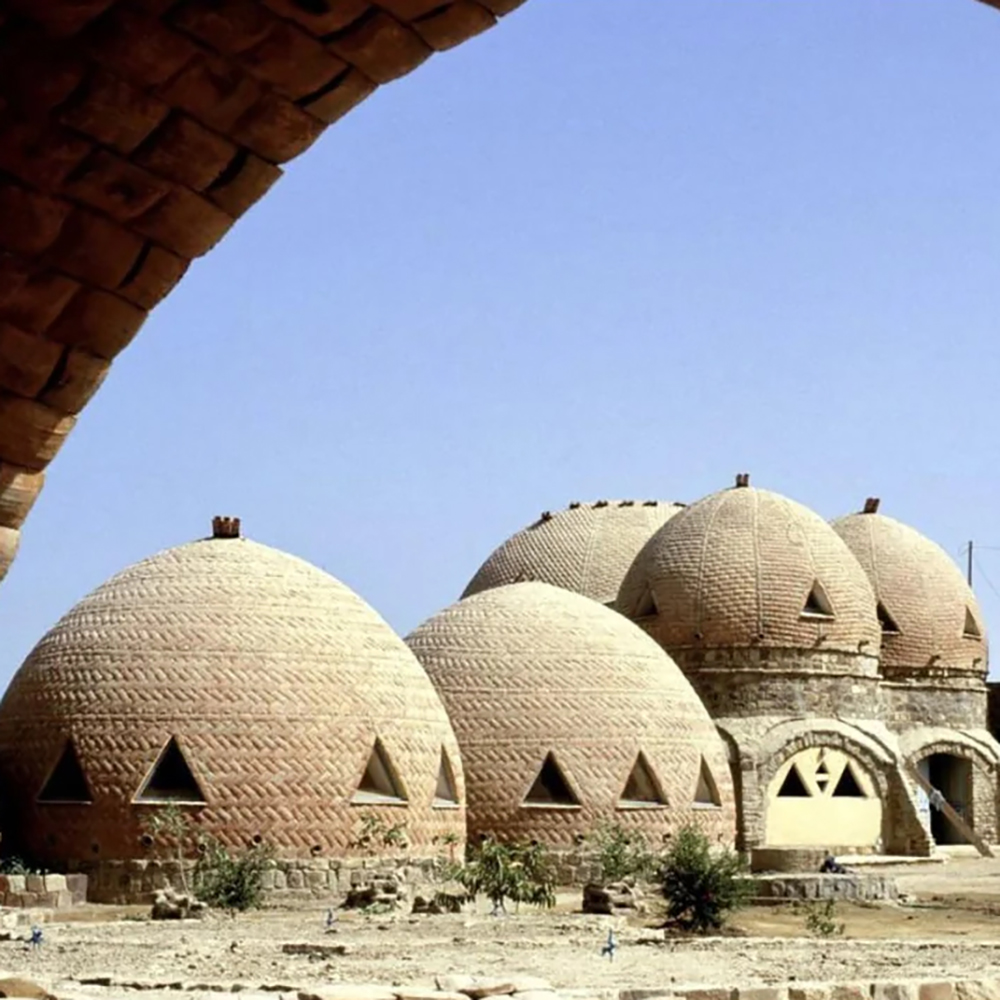
Kaedi is located in a remote sector of Mauritania, near the border of Senegal. Its hospital serves a rural population. The extension adds 120 beds to the hospital, an operating theatre complex, paediatric, surgical, and ophthalmic departments, a maternity and general medical unit, a laundry, kitchens, storerooms, a garage, and a workshop. The architects were not to replicate the earlier hospital’s conventional concrete-frame buildings; their brief was to house the planned facilities by developing new low-cost techniques of construction employing local materials and skills that would be applicable to other building types within the region. All workmen were local, trained on the site to perform the new techniques. Although the use of brick is not a part of the local vernacular, the architects chose to develop a structural vocabulary of handmade brick, fired in kilns built near the source of clay. The structural repertoire that emerged, after on-site experimentation with a number of domes and vaults, included simple domes, complex domes, conventional half-domes, pod-shaped spaces, and self-supporting pointed arches, which form winding circulation corridors. The overall plan for the hospital extension was derived from these forms. Adequate natural light enters the complex through glass blocks set into the brickwork and from interstices left between the brick arches. The response of both doctors and patients has been positive, and the community takes pride in the fact that the medical facility was built by their own people. The jury believes that the innovative construction techniques introduced may have wide significance, particularly since the successful functioning of the hospital should encourage similar initiatives elsewhere.
Kaedi se encuentra en una zona remota de Mauritania, cerca de la frontera con Senegal. Su hospital atiende a una población rural. La ampliación añade 120 camas al hospital, un complejo de quirófanos, departamentos de pediatría, cirugía y oftalmología, una unidad de maternidad y medicina general, lavandería, cocinas, almacenes, garaje y taller. Los arquitectos no debían replicar los edificios convencionales de estructura de hormigón del hospital original; su objetivo era albergar las instalaciones previstas desarrollando nuevas técnicas de construcción de bajo coste, utilizando materiales y mano de obra locales, que fueran aplicables a otros tipos de edificios en la región. Todos los trabajadores eran locales y fueron capacitados en la obra para aplicar las nuevas técnicas. Aunque el uso del ladrillo no forma parte de la arquitectura tradicional local, los arquitectos optaron por desarrollar un lenguaje estructural a base de ladrillos hechos a mano, cocidos en hornos construidos cerca de la fuente de arcilla. El repertorio estructural resultante, tras la experimentación in situ con diversas cúpulas y bóvedas, incluyó cúpulas simples, cúpulas complejas, semicúpulas convencionales, espacios con forma de vaina y arcos apuntados autoportantes que conforman sinuosos pasillos de circulación. El plan general de la ampliación del hospital se derivó de estas formas. La luz natural entra en el complejo a través de bloques de vidrio insertados en la mampostería y de los intersticios dejados entre los arcos de ladrillo. La respuesta tanto de médicos como de pacientes ha sido positiva, y la comunidad se enorgullece de que el centro médico haya sido construido por su propia gente. El jurado considera que las innovadoras técnicas de construcción introducidas pueden tener una gran relevancia, sobre todo porque el buen funcionamiento del hospital debería fomentar iniciativas similares en otros lugares.
Text via the Aga Khan Development Network (AKDN) for the Aga Khan Award for Architecture.